

Background. Approximately 70% of newly diagnosed chronic lymphocytic leukemia (CLL) patients present in early Binet or Rai stage, may never require treatment, and may have a life expectancy similar to that of the general population. Two independent and recent studies have identified the clinical and immunogenetic variables associated with shorter time to first treatment (TTFT) in Binet A and Rai 0 CLL (Condoluci et al., Blood 2020; Cohen et al., Haematologica 2020). However, the clinical impact of gene mutations in predicting TTFT is not completely understood.
Purpose. Using a training/validation approach, we aimed at identifying new molecular biomarkers that may predict early treatment requirement and may help clinicians to better plan the watch and wait strategy in asymptomatic early stage CLL patients.
Methods. The training cohort included 295 CLL in Binet A stage who did not require treatment for at least 3 months after diagnosis. The two validation multicenter cohorts included 402 treatment-naïve Binet A CLL patients (Binet A validation cohort) and 395 untreated Rai 0 CLL patients (Rai 0 validation cohort), respectively. In the training cohort, tumor genomic DNA was isolated from peripheral blood mononuclear cells at the time of diagnosis and was analyzed in the coding exons plus splice sites of the most frequently mutated genes in CLL with a next-generation-sequencing (NGS) approach using a variant allele frequency (VAF) threshold of 5%. In the validation series, the XPO1 gene (exons 15 and 16) was analyzed by NGS or by Sanger sequencing. The primary endpoint was TTFT defined as the time interval between the date of CLL diagnosis and the date of first CLL treatment.
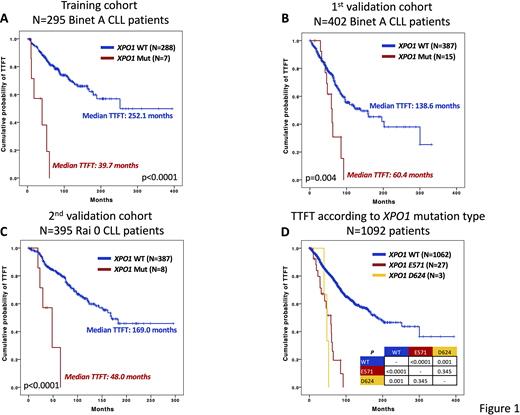
Results. In the training cohort, NGS mutational analysis showed that XPO1 was mutated in 7 (2.4%) patients. In univariate analysis, trisomy 12 (HR 2.42; 95% CI 1.43-4.15; p=0.001), unmutated IGHV genes (HR 4.51; 95% CI 2.83-7.05; p<0.0001) and mutations of XPO1 (HR 8.88; 95% CI 3.77-20.95; p<0.0001) (Fig. 1A), NOTCH1 (HR 3.02; 95% CI 1.66-5.51; p<0.001) and SF3B1 (HR 2.65; 95% CI 1.15-6.10; p=0.022) were associated with a shorter TTFT. By multivariate analysis, XPO1 mutations (HR 4.24; 95% CI 1.72-10.44; p=0.002) and unmutated IGHV genes (HR 3.43; 95% CI 2.08-5.67; p<0.0001) maintained an independent association with a shorter TTFT. XPO1 mutational analysis was subsequently investigated in 2 independent multicenter cohorts of early stage CLL patients. In the Binet A validation cohort (N=402 patients), XPO1 was mutated in 15 (3.7%) patients and was associated with a shorter TTFT (HR 2.59; 95% CI 1.36-4.96; p=0.004) (Fig. 1B). Similarly, also in the Rai 0 validation cohort, (N=395 patients), XPO1was mutated in 8 (2.0%) patients and was associated with a shorter TTFT (HR 6.02; 95% CI 15.03-4.96; p<0.001) (Fig. 1C). Moreover, in the Rai 0 validation cohort, XPO1 mutations maintained an independent association with a shorter TTFT when corrected in multivariate analysis by the IGHV mutational status (HR 3.31; 95% CI 1.30-8.44; p=0.012). By combining the training and the validation cohorts (N=1092 patients), a total of 30 somatically acquired XPO1 mutations were identified (2.7% of patients). More precisely, 27 (90.0%) mutations affected XPO1 codon E571 and 3 (10.0%) codon D624. This finding suggests that a target sequencing or an allele-specific polymerase chain reaction based method may be used to identify XPO1 mutations in a simple and time-effective manner. From a clinical perspective, patients carrying either XPO1 E571 or D624 mutations showed superimposable outcome in terms of TTFT (p=0.345) (Fig. 1D).
Conclusions. Mutations of the XPO1 gene, encoding for exportin 1 which mediates the nuclear export of proteins and RNAs, are an independent predictor of shorter TTFT validated in independent series of early stage treatment-naïve CLL patients. XPO1 mutations are conceivably gain-of-function and may enhance cell proliferation by exporting out of the nucleus with a greater extent proteins that physiologically downregulate cell proliferation. Based on these results, XPO1 mutational analysis might be incorporated in other prognostic scores and help clinicians to refine the management of the watch and wait strategy for early stage CLL. In addition, XPO1 inhibitors are particularly active in XPO1E571 mutated cells (Taylor et al., Cancer Discov 2019) providing initial pre-clinical rational for their usage in XPO1 mutated CLL patients.
Scarfo:AstraZeneca: Honoraria; Gilead: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Abbvie: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Del Giudice:AstraZeneca: Membership on an entity's Board of Directors or advisory committees; Roche: Other: grant for meeting partecipation; Janssen: Other: grant for meeting participation; Tolero: Membership on an entity's Board of Directors or advisory committees. Sportoletti:Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Abbvie: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Marasca:Shire: Honoraria; Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Abbvie: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Roche: Membership on an entity's Board of Directors or advisory committees. Ghia:Acerta/AstraZeneca: Consultancy, Honoraria; ArQule: Consultancy, Honoraria; Gilead: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company), Research Funding; BeiGene: Consultancy, Honoraria; Janssen: Consultancy, Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company), Research Funding; Novartis: Research Funding; Celgene/Juno: Consultancy, Honoraria; Lilly: Consultancy, Honoraria; MEI: Consultancy, Honoraria; Sunesis: Consultancy, Honoraria, Research Funding; Adaptive, Dynamo: Consultancy, Honoraria. Foà:Roche: Membership on an entity's Board of Directors or advisory committees; Incyte: Speakers Bureau; Roche: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Novartis: Speakers Bureau; Abbvie: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Gaidano:Sunesys: Membership on an entity's Board of Directors or advisory committees; Abbvie: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Astrazeneca: Membership on an entity's Board of Directors or advisory committees. Rossi:AstraZeneca: Honoraria, Research Funding; Janssen: Honoraria, Research Funding; Gilead: Honoraria, Research Funding; Abbvie: Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal